
When Is It ADHD and When Is It Just Childhood?
What research on attention, impulsivity, and self-regulation reveals about how children grow, learn, and focus.

I was interrupted no less than four times trying to write this paragraph: once for hugs, once for a Magna-Tile emergency, and twice for reasons I still don’t fully understand. My kids regularly lose water bottles, forget homework folders, and bounce between projects like they’re running their own experimental design lab in chaos.
These everyday moments — the spills, the forgetfulness, the ten-second attention span — are part of what we call typical development. The ability to sustain focus, plan ahead, and inhibit impulses is still wiring up in early childhood. But for some kids, those skills don’t just lag; they struggle to click into place, showing up as the chronic distractibility and impulsivity of ADHD.
ADHD affects about 3–9% of school-aged children worldwide, depending on how it’s measured and which criteria are used (Ogundele & Ayyash, 2023). That means almost every classroom includes at least one or two students whose attention challenges go beyond what’s typical for their age.
During ADHD Awareness Month, it’s worth pausing to clarify how developmental psychology helps us distinguish fleeting distractibility from deeper patterns of attentional dysregulation that can interfere with learning, relationships, and well-being.
As a quick note: I’m a developmental psychopathologist and science communicator who studies the development of emotional and behavioral problems in children. I’m not a clinician or medical provider, and this post is for educational purposes only.
Key Concepts
Attention-Deficit/Hyperactivity Disorder (ADHD): A neurodevelopmental condition involving persistent patterns of inattention, hyperactivity, and/or impulsivity that interfere with daily life at home, school, or in relationships.
Inattention: Difficulty sustaining focus, following through on tasks, or organizing activities. This often looks like daydreaming, careless mistakes, or forgetfulness rather than defiance.
Hyperactivity and Impulsivity: High levels of movement or restlessness that go beyond what’s expected for a child’s age (e.g., fidgeting, talking excessively, or having trouble staying seated).
Executive Function: The brain’s self-management system (e.g., working memory, inhibition, and cognitive flexibility) that allow us (yes, even adults!) to plan, focus, and control impulses. Many ADHD symptoms reflect lagging executive-function development rather than lack of willpower.
Research Spotlight
The American Academy of Pediatrics (AAP, 2019) and the DSM-5-TR (APA, 2022) emphasize that ADHD diagnosis must meet the following criteria:
Symptoms persist for at least six months
Six or more symptoms of inattention and/or hyperactivity-impulsivity for children up to age 16 years
They are inconsistent with the child’s developmental level
They cause impairment in two or more settings (e.g., school and home)
That last point (two or more settings) matters enormously.
A child who melts down during math but focuses for hours on Legos might not have ADHD; they’re struggling with task-specific frustration or motivation.
Another child who loses track of multi-step instructions, interrupts conversations, and forgets belongings both at home and school shows a cross-context pattern that raises red flags.
What Research Shows
Consistency across environments is one of the clearest indicators of ADHD.
This usually means the behaviors are seen at home, in the classroom, and in peer interactions. In their 2021 study, Jungersen and Lonigan (2021) examined parent and teacher reports of ADHD symptoms and found only moderate agreement between them, reflecting how context can shape what adults observe.
Teacher ratings tended to align more closely with objective measures of attention control, suggesting that difficulties consistent across both structured (school) and unstructured (home) environments are more clinically meaningful than those limited to a single context.
Executive-function differences help explain these patterns.
Children with ADHD often show weaker working memory and inhibitory control on average (Best & Miller, 2010; Best et al., 2009). That means they may know the rules but struggle to apply them consistently — like remembering multi-step directions or resisting impulse actions when excited.
It’s important to also know that these aren’t just behavior differences. They reflect real, measurable differences in the brain, as shown by structural and functional MRIs (see
’s post on this too).Children (and adults) with ADHD tend to have smaller volume in areas tied to executive functioning, like the prefrontal cortex and hippocampus (Hoogman et al., 2017). I like to explain these as the brain’s “brake pedal.”
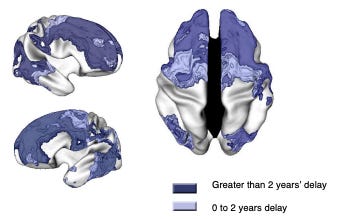
These regions also mature more slowly than neurotypical children (~3 years later) which is partially why symptoms may lessen with age (Shaw et al., 2007).

From Shaw et al. (2007). These are regions where the ADHD group had delayed brain maturation. But Shaw’s team also found something interesting: while attention and control regions develop more slowly, the motor cortex develops faster (aka, the brain’s “gas pedal”). In their sample, kids with ADHD hit peak development in this movement-focused area a few months earlier than peers.

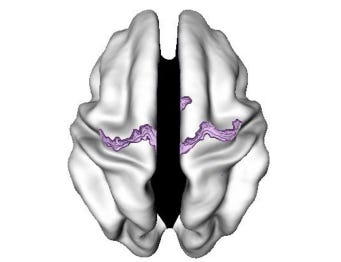
From Shaw et al. (2007). Regions where the ADHD group had early cortical maturation (this region mostly the motor cortex).
In other words, the parts of the brain that get kids moving mature before the parts that help them slow down — the “go” system races ahead of the “control” system.
These findings suggest that ADHD isn’t just about distractibility; it’s about a timing difference in how and when the brain’s executive systems mature and coordinate attention.
Typical vs. Atypical Attention in Preschoolers
Preschoolers naturally exhibit high activity levels and short attention spans - it’s developmentally appropriate. But in ADHD, these behaviors are more frequent, intense, and persistent than expected (APA, 2022).
For example, all 4-year-olds may interrupt occasionally; a child with ADHD interrupts dozens of times, daily, across contexts and this interferes with the child’s functioning daily (not parents’ daily functioning where we feel overstimulated from not being able to finish a thought all day 😉).
Inattentive Form: Children with predominantly inattentive ADHD are often overlooked early on because their symptoms are quieter: daydreaming, seeming “off in their own world,” or taking longer to complete work.
They may not disrupt the classroom, so difficulties often become more apparent only when academic or organizational demands increase.
de la Peña et al. (2020) note that this presentation is frequently underrecognized and undertreated compared to more overtly hyperactive forms.
In other words: distraction, forgetfulness, and impulsivity exist on a continuum. ADHD is diagnosed when those tendencies are developmentally atypical, cross settings, and create functional impairment — not when they simply frustrate adults.
Why It Matters
To avoid overdiagnosis: There’s a risk of labeling energetic but healthy children as “disordered,” leading to unnecessary stigma and intervention. A nuanced understanding helps prevent misclassification.
To ensure early and appropriate support: When children truly cross that threshold, early recognition allows for interventions that can change trajectories.
To guide caregivers and teachers: Many adults wonder, “Is this just a stage?” Clear criteria help decide when to adjust routines versus when to seek help.
To allocate resources wisely: Schools and pediatric systems often face stretched supports; good diagnostic precision ensures they reach the right children.
To reduce stigma: Emphasizing that attention varies along a continuum — and that ADHD is not “bad behavior” — fosters compassion and inclusion.
Long Story Short
Distinguishing between “a naturally distractible child” and “a child with ADHD” means paying attention to patterns, persistence, and context. ADHD isn’t defined by occasional forgetfulness or bursts of energy — it’s a long-term, cross-setting pattern that consistently interferes with daily life.
Quick Takeaways
ADHD diagnosis requires more than symptoms: it involves impairment, duration, and consistency across settings.
Age norms matter: what’s “too distractible” for a 3-year-old is different from what’s expected in a 10-year-old.
Inattentive-type ADHD can be easy to miss early on because it looks quiet rather than disruptive.
Neuroimaging and connectivity research provide supporting (not definitive) biological markers.
Good practice integrates multiple informants (parents, teachers), detailed history, and rule-outs of overlap conditions (e.g. anxiety, learning disorders).
Balancing caution about overlabeling with compassion for those truly struggling ensures kids get the right kind of support.
Have you ever wondered whether your child’s distractibility was “just childhood” or something more? What patterns or clues have you noticed across home and school?
Development Decoded is built on a simple belief: science should be clear, practical, and accessible to anyone who cares about kids. I write, research, and create resources outside of my day job and family life to make that happen. If you’d like to help fuel the work, you can now do so with one coffee at a time.
References
American Psychiatric Association (2022). Diagnostic and statistical manual of mental disorders, fifth edition, text revision. Washington: American Psychiatric Association.
Best, J. R. & Miller, P. H. (2010). A developmental perspective on executive function. Child Development, 81(6). https://doi.org/10.1111/j.1467-8624.2010.01499.x
Best, J. R., Miller, P. H., & Jones, L. L. (2009). Executive Functions after Age 5: Changes and Correlates. Developmental Review, 29(3), 180–200. https://doi.org/10.1016/j.dr.2009.05.002
de la Peña, I. C., Pan, M. C., Thai, C. G., & Alisso, T. (2020). Attention-Deficit/Hyperactivity Disorder Predominantly Inattentive Subtype/Presentation: Research Progress and Translational Studies. Brain sciences, 10(5), 292. https://doi.org/10.3390/brainsci10050292
Jungersen, C. M., & Lonigan, C. J. (2021). Do Parent and Teacher Ratings of ADHD Reflect the Same Constructs? A Measurement Invariance Analysis. Journal of psychopathology and behavioral assessment, 43(4), 778–792. https://doi.org/10.1007/s10862-021-09874-3
Hoogman, M., Bralten, J., Hibar, D. P., Mennes, M., Zwiers, M. P., Schweren, L. S. J., van Hulzen, K. J. E., Medland, S. E., Shumskaya, E., Jahanshad, N., Zeeuw, P., Szekely, E., Sudre, G., Wolfers, T., Onnink, A. M. H., Dammers, J. T., Mostert, J. C., Vives-Gilabert, Y., Kohls, G., Oberwelland, E., … Franke, B. (2017). Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: a cross-sectional mega-analysis. The Lancet Psychiatry, 4(4), 310–319. https://doi.org/10.1016/S2215-0366(17)30049-4
Ogundele, M. O., & Ayyash, H. F. (2023). ADHD in children and adolescents: Review of current practice of non-pharmacological and behavioural management. AIMS Public Health, 10(1), 35–51. https://doi.org/10.3934/publichealth.2023004
Shaw, P., Eckstrand, K., Sharp, W., Blumenthal, J., Lerch, J. P., Greenstein, D., Clasen, L., Evans, A., Giedd, J., & Rapoport, J. L. (2007). Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proceedings of the National Academy of Sciences of the United States of America, 104(49), 19649–19654. https://doi.org/10.1073/pnas.0707741104
Wolraich, M. L. et al. (2019). Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 144(4): e20192528. https://doi.org/10.1542/peds.2019-2528
Another great read! Thank you :) can you cover ODD next?
I just found your Substack and want to tell you that love it so much. Subscribed and can't wait for it to start hitting my inbox! Lol never thought I'd say that! 😆❤️